Chew gum and I'll cancel your surgery
Fasting, compassion and evidence
As clinicians we are often expected to follow practices that are 'known' to be beneficial. It is widely expected by the public that what we say is based on evidence and is indeed 'best'.
It has long been considered good practice to restrict oral intake prior to surgery, in fact a quote attributable to Lord Lister in 1882 goes as such >"While it is desirable that there should be no solid matter in the stomach when chloroform is administered, it will be found very salutary to give a cup of tea or beef-tea about two hours previously"
This was about to change significantly in 1946 when Mendelson described a case of aspiration of stomach contents in obstetric and labouring patients. 1 The particular patient were undergoing general anaesthesia and were not intubated. This would change the world for the majority of surgical patients for the next 50 years. Nil by mouth from midnight became the mantra and, sadly, this will be all too familiar to many reading this post.
I know best now do as I say!
The thing that spurred this post for me was a post I saw on Facebook by a relatively light hearted 'personality' on the internet - The Anaesthetic Registrar. The Anaesthetic Registrar is a fictitious character that is in fact a collection of ever changing anonymous individuals across the globe who post, often, satirical comments on the frustrations of their daily practice. This week I notice this comment: 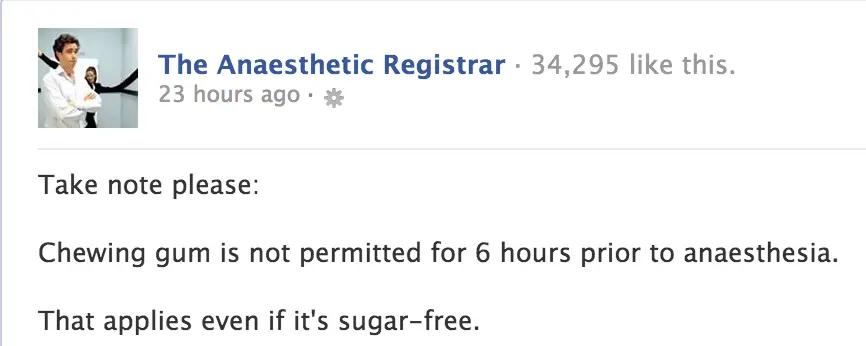
I was immediately taken aback by the lack of compassion and also the fact that it was so far away from my understanding of contemporary practice in preoperative fasting.
The responses from others really shocked me. I've removed the images and the individuals names, but am sharing the content of their posts. Take this example:

I'm the boss and you'll do what I say, because I say so.
 This one was by far the most shocking in my opinion, not only was the individual's ideation lacking in any good evidence base, but they actually seemed to take pleasure in humiliating a patient at a time of great stress. The individual even points out that 'the anaesthetist was shocked, as was the surgeon' and I have to wonder if they were shocked that the patient was consuming a tic tac or by the behaviour of the anaesthetic nurse.
This one was by far the most shocking in my opinion, not only was the individual's ideation lacking in any good evidence base, but they actually seemed to take pleasure in humiliating a patient at a time of great stress. The individual even points out that 'the anaesthetist was shocked, as was the surgeon' and I have to wonder if they were shocked that the patient was consuming a tic tac or by the behaviour of the anaesthetic nurse.
As the debate progressed, some people began to share some evidence that studies has shown chewing gum does not cause any harm, in fact it has been shown to improve gastric emptying and reduce stomach content acidity (two of the primary aims of fasting!). 2
Have Things Changed?
Considering contemporary anaesthesia practice there are numerous changes that have a very significant impact on preoperative fasting. Let's consider but a few:
- It would be very unusual these days for an obstetric patient to have anaesthesia without intubation
- We no longer use chloroform or ether
- The use of suxamethonium (Scoline) is much rarer these day with the growth in popularity of reversible muscle relaxant such as rocuronium
- Securing a patients airway is one of the highest priorities for anaesthesia providers and where there is an increased risk of aspiration / regurgitation / vomiting, standard practice would be the use a cuffed endo-tracheal tube
- The rates of aspiration have dropped significantly, with a rate of 0.0006% in 2002. 3
Now clearly this is not a complete discussion of the changes, there are so many more advances in practice these days and yet there still appears to be a huge resistance to allowing patients to fast for shorter periods of time. A 2002 study found that 91% of patients were fasted from midnight. 4 There have been numerous later studies which have shown very large discrepancies between evidence based guidance and the reality for patients.
Randomized trials, meta-analyses, case control studies and even MRI imaging studies of gastric emptying have consistently shown that the consumption of clear fluids up to 2 hours prior to surgery is both safe and comforting for patients.5,6 Even the belief that consuming milk is bad is being challenged, with gastric emptying times being show to have no difference for coffee with milk vs coffee without milk, verified by ultrasound studies. 7
What Should We Be Doing?
I think it is clear from the literature that the nil by mouth from midnight practice is well and truly ready to be discarded. What is the recommended practice? Well that's where things get a little complicated. Most national anaesthesia bodies have recommendations on the subject - Australian and New Zealand College of Anaesthetists, American Society of Anaesthesiologists, Royal College of Anaesthetists - certainly do. Following the guidance set out by your national governing body shouldn't present too much controversy!
It may well be necessary to build support for any change within you local department and team. Present the evidence, discuss it, challenge opinions. In a quote of questionable origin it is stated that: >The plural of anecdote is not data
I think this serves as a great starting point for a discussion on the rational basis for exploration of fasting practices. A great discussion of anecdote in medicine is available here
The Final Reason
If you ever want to convince yourself of the merits of shortening fasting times, try this little experiment.
- Eat your evening meal and go to bed.
- The following morning take yourself to a place you really don't want to be
- Don't allow yourself anything to eat or drink
- Restrict your movements and provide as little distraction as possible
- Ensure that you are particularly worried about something
- Focus on the worry and then consider that the only way to deal with your problem is to hand over complete control over whether you live or die to a group of complete strangers.
Are you feeling upset yet?
1 Mendelson CL. The aspiration of stomach contents into the lungs during obstetric anaesthesia. American Journal of Obstetrics and Gynecology. 1946;52:191-205.
2 Dubin S, Jense H, McCranie J, Zubar V. Sugarless gum chewing before surgery does not increase gastric fluid volume or acidity. Canadian Journal of Anaesthesia. 1994;41(7):603-6.
3 Fasting S, Gisvold SE. [Serious intraoperative problems--a five-year review of 83,844 anesthetics]. Canadian Journal of Anaesthesia = Journal Canadien D'Anesthesie. 2002;49(6):545-53.
4 Crenshaw JT, Winslow EH. Preoperative fasting: old habits die hard. American Journal of Nursing. 2002;102:36-44.
5 Aguilar-Nascimento JE, Dock-Nascimento DB. Reducing preoperative fasting time: A trend based on evidence. World Journal of Gastrointestinal Surgery. 2010;2(3):57-60.
6 Schmitz A, Kellenberger CJ, Liamlahi R, Studhalter M, M W. Gastric emptying after overnight fasting and clear fluid intake: a prospective investigation using serial magnetic resonance imaging in healthy children. British Journal of Anaesthesia. 2011;107(3):425-9.
7 Hillyard S, Cowman S, Ramasundaram R, Seed PT, O'Sullivan G. Does adding milk to tea delay gastric emptying? British Journal of Anaesthesia. 2014;112(1):66-71.